Last Updated on June 9, 2024 by Birth Facts
For most medical procedures, medical professionals are required to inform patients of the risks of different options, and patients have to give informed consent to any procedures. Birth is not like this. Women are systematically denied information about the risks of different birth options.
This website sets out the risks of all modes of delivery – standard vaginal, ventouse, forceps, and c-section. We have no stance on which of these options you should take. Deciding how you want to give birth is a personal decision that depends on what is important to you. Your partner, family, friends, doctor or midwife can discuss your options with you.
Ultimately, you and you alone have the right to decide how you give birth.
The supporting evidence for the data on this page is here.
What are the main birth options?
The main birth options for women are:
- Unassisted vaginal birth
- Forceps
- Ventouse or vacuum-assisted
- Planned caesarian section or c-section
- Unplanned c-section
Unassisted vaginal delivery involves delivering the baby through the vagina without the use of instruments such as forceps or vacuums.
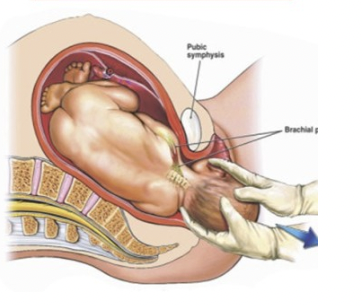
Sometimes during active labour, it may not be possible to have an unassisted vaginal delivery without posing large risks to mother or baby. Also, labour might just not be progressing and the mother may be exhausted after a long labour. In that case, women will either deliver via forceps, vacuum or unplanned c-section.
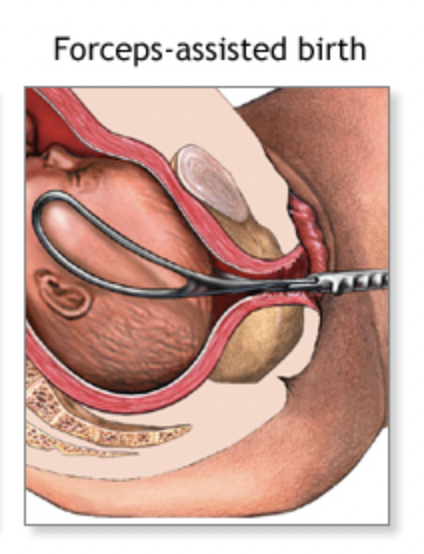
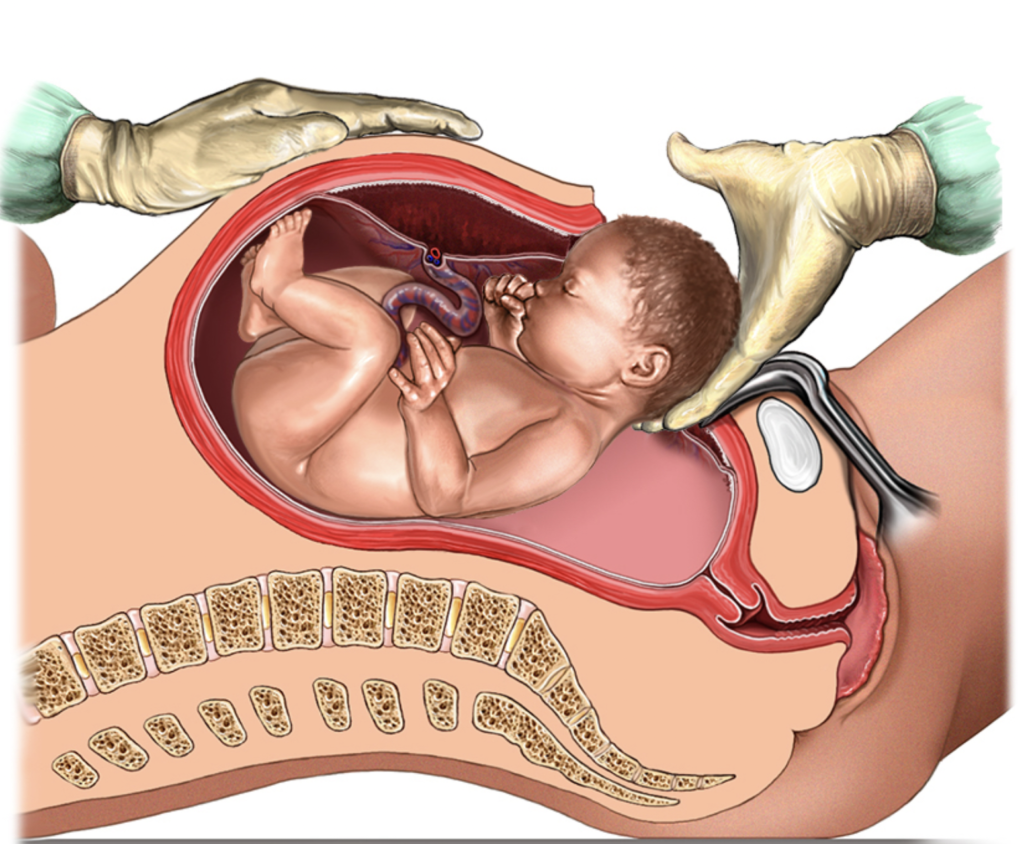
Forceps are metal implements around the size of large salad tongs that are clamped to the side of the baby’s head. The baby is then pulled out using the forceps:
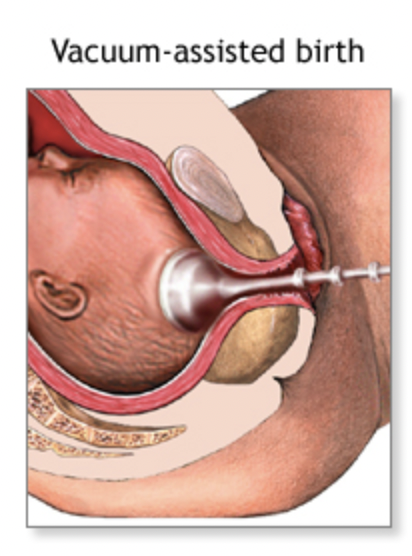
Ventouse or vacuum-assisted birth involves placing a soft suction cup on baby’s head which stays in place by suction:
Caesarian section or c-section involves delivering the baby by cutting into the mother’s abdomen. The uterus is then opened with a second cut and the baby is delivered. The cut is then stitched together.
There are two different types of c-section delivery: (1) planned c-section, and (2) unplanned c-section.
Planned c-section is usually done from the 39th week of pregnancy and is performed prior to labour.
Unplanned (sometimes called ’emergency’) c-section is done during labour if it is thought that a vaginal birth would be too risky for mother or baby, or if the women decides to have a c-section during labour. It is ‘unplanned’ in the sense that the woman tried to give birth vaginally but decided to have a c-section during labour.
How many people choose each mode of delivery?
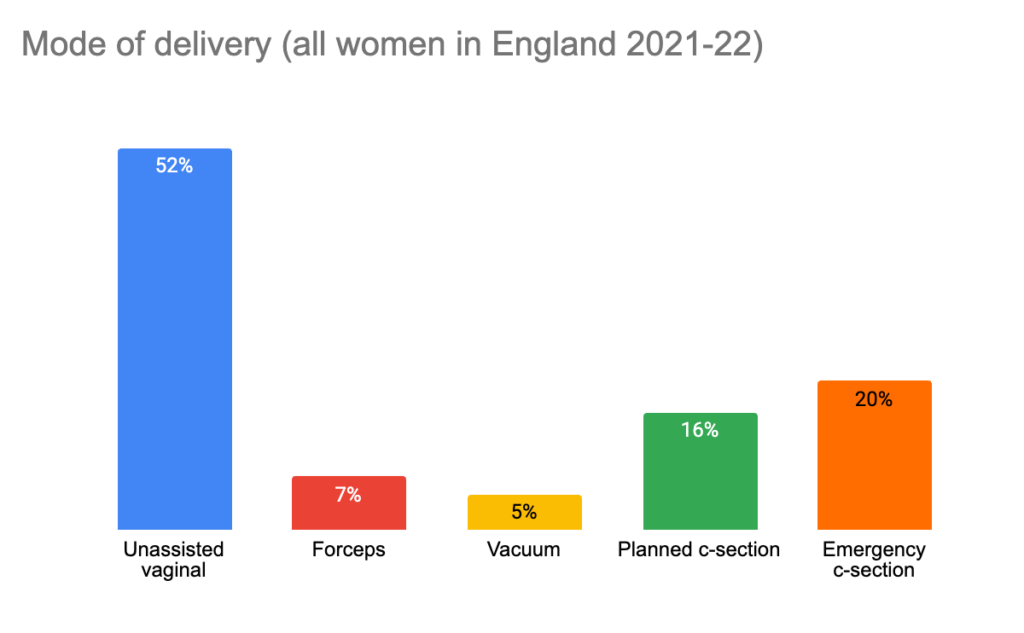
Modes of delivery in English women from 2021 and 2022 broke down as follows:
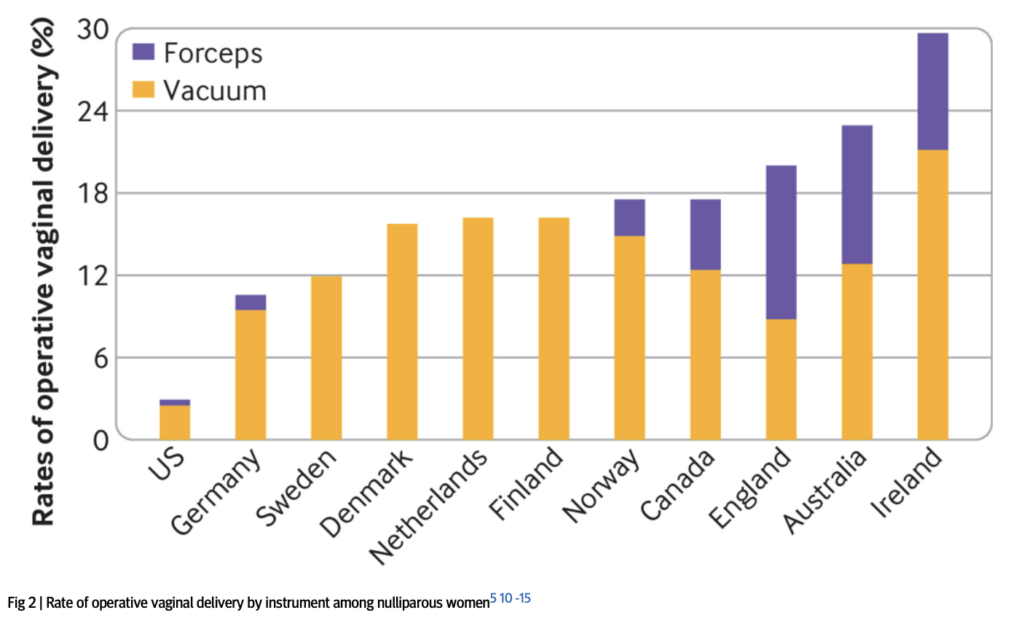
However, the rate of different modes of deliveries varies significantly across rich countries. Different countries take very different approaches to c-section, forceps and ventouse. For example, in Cyprus, more than half of births are by c-section, compared to only 15% in Iceland. In some countries, such as Sweden, Denmark and Finland, forceps are never used, whereas in England they account for more than half of operative deliveries:
The effect of age on mode of delivery
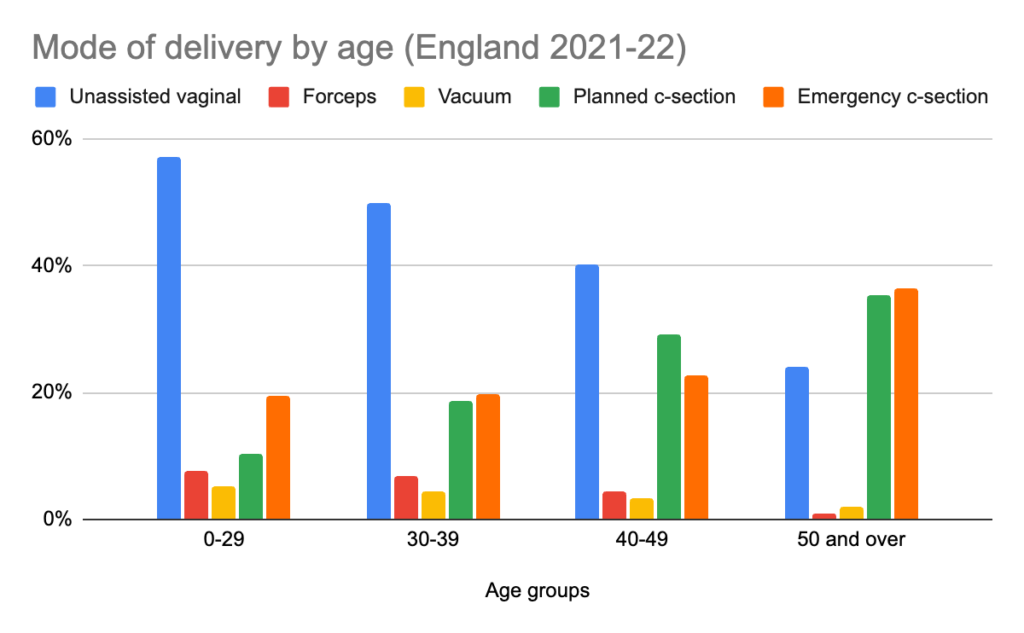
The chance that you will be able to have an unassisted delivery decreases with age. The rate of c-section increases with age. For example, mode of delivery for different age groups giving birth in England from 2021-22 is shown below:
This general pattern holds across all countries.
Your birth plan
A birth plan is a record of what you would like to happen during your labour and after the birth. You don’t have to create a birth plan, but you can if you would like. Your birth plan is personal to you. It depends on what you want, your medical history, your circumstances and what is available at your maternity service.
Your birth plan needs to plan two decisions: (1) prior to labour, whether you aim to have a planned c-section or an unassisted vaginal birth, (2) if you plan to have an unassisted vaginal birth but are not able to, whether you have forceps, vacuum or unplanned c-section. Many women who try to have an unassisted vaginal birth are not able to do so, and only find this out during labour. It is therefore important to consider what you want to do if you cannot have your ideal birth.
Although making a birth plan can be useful, since you have the right to decide how to give birth, you also have the right to change your mind during labour.
More details on creating a birth plan are available from the UK National Health Service here.
What are the risks of different modes of delivery to women?
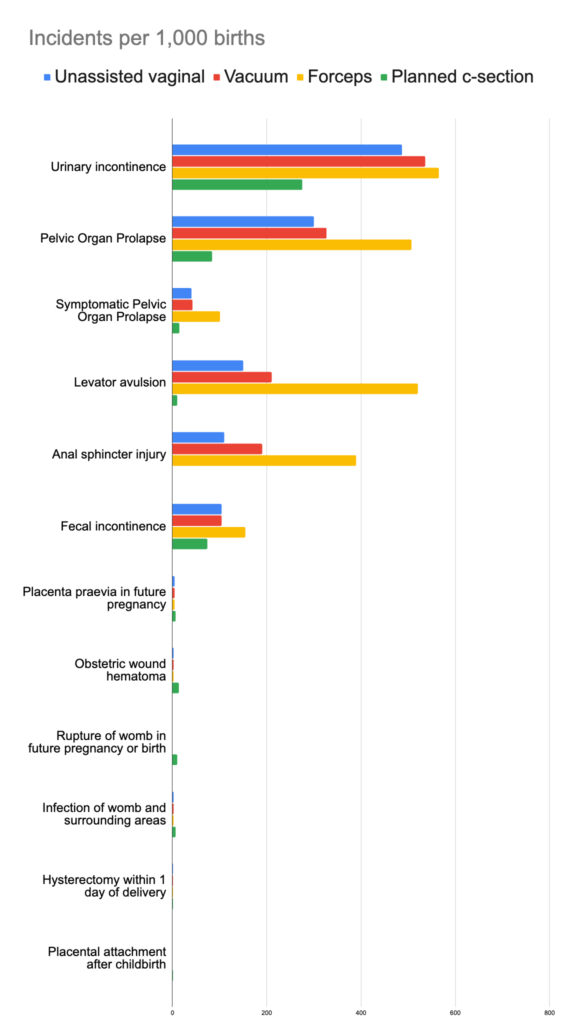
All birth options carry risks. In order to make an informed decision about their birth options, women need to know how large these risks are. The chart below summarises these risks for typical women in rich countries:
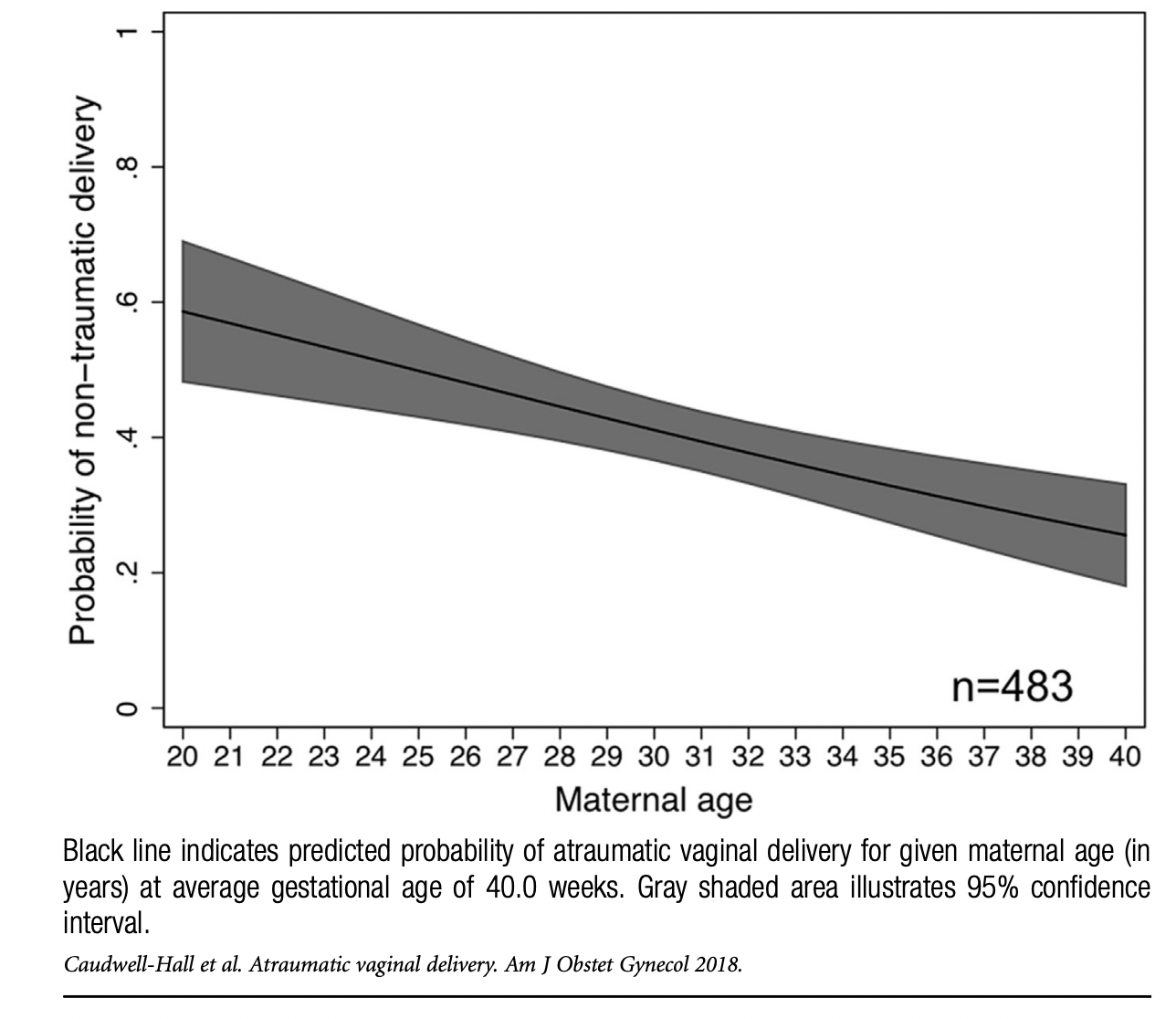
The effects of age on birth trauma
The risk of traumatic delivery (one that involved injury to the perineum, levator avulsion, or anal sphincter injury) increases with age. A 20 year old woman has a 60% chance of a non-traumatic vaginal delivery, whereas a 35 year old has only a 1 in 3 chance.
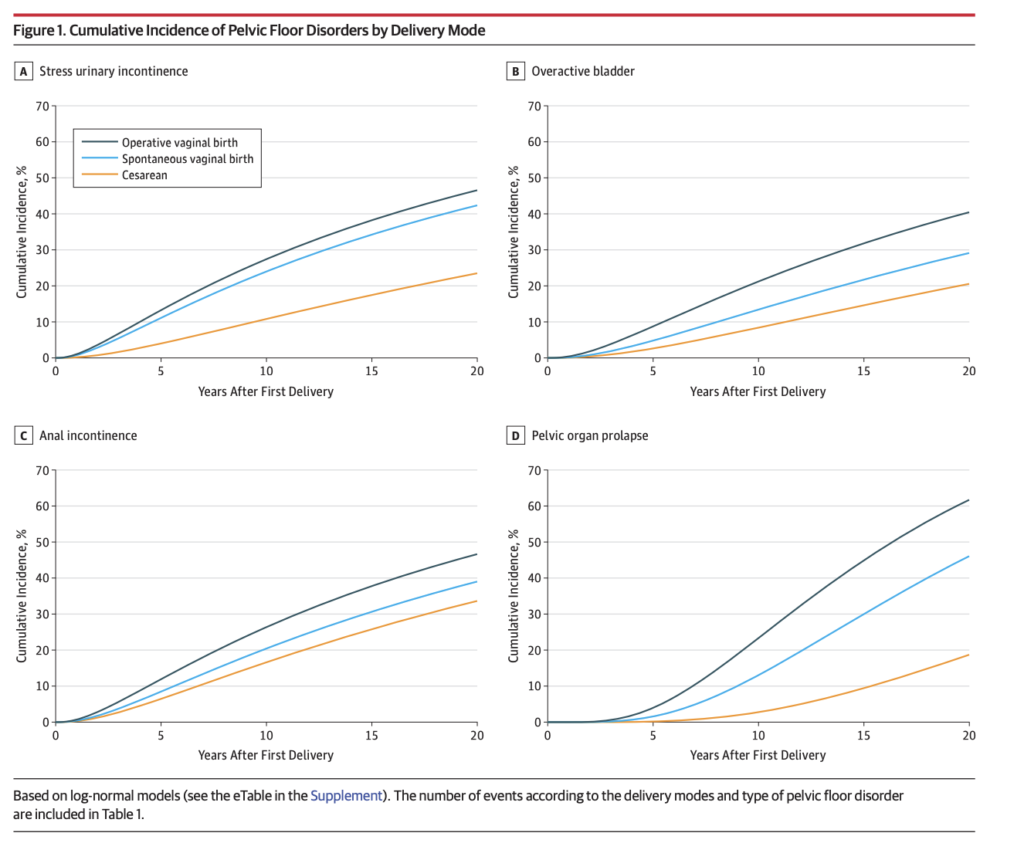
For women who have given birth, the risk of suffering key pelvic floor disorders increases with age. The chart below shows one estimate of the combined effect of age and mode of delivery on pelvic floor disorders.
Reviewing the risks in detail
Deciding which birth option to choose is a personal decision. You can make an informed choice by comparing the risks associated with different birth choices and deciding what matters to you most. For further guidance and discussion, you can discuss your options with your partner, family, friends, doctor or midwife. Ultimately, you and you alone have the right to decide how you give birth.
In order to make informed decisions, women need to know not only the probability of different outcomes but also how bad those outcomes are. The rest of this page outlines how bad those outcomes are. The outcomes are discussed in order of how likely they are to occur, not in order of how bad they are.
Pain
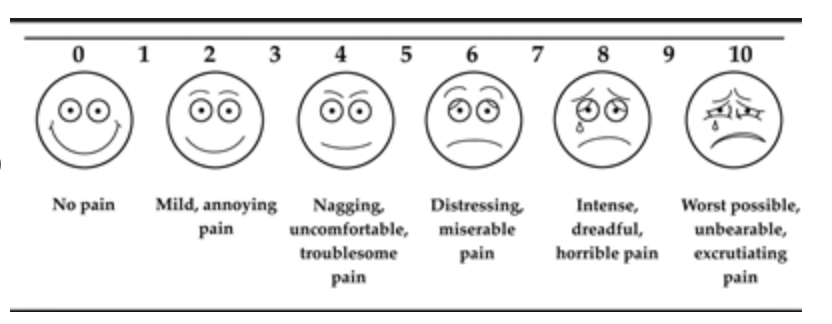
The amount of pain varies across different modes of delivery and depends on when pain is measured. A study by Schindl et al (2003) asked women to rate their levels of pain on 11 point scale similar to the one below: 0 means no pain, 5 means moderate pain, and 10 means the worst-possible pain.
The chart below shows levels of pain experience by the typical woman in the study during birth, 4 days after birth and 4 months after birth. The typical woman delivering vaginally (whether unassisted or with forceps or vacuum) did not have an epidural, which is by far the most effective form of pain relief.
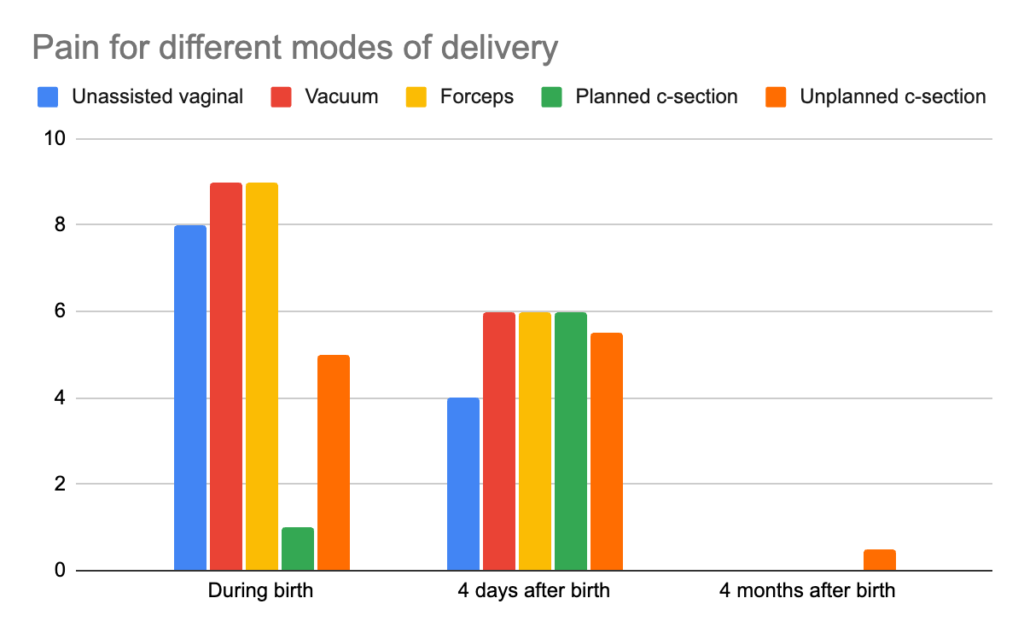
During birth, vaginal birth involves extreme pain, unplanned c-sections involve moderate pain, and planned c-sections involve little pain. Four days after birth, levels of pain are similar across all types of birth, though somewhat lower for unassisted vaginal. Four months after birth, pain is low for all modes of birth.
Urinary Incontinence
There are two kinds of urinary incontinence. Stress urinary incontinence is leakage of urine during moments of physical activity, such as coughing, sneezing, laughing, or exercise. Urge urinary incontinence occurs when there is an involuntary loss of urine associated with a sudden and compelling desire to pass urine.
Urinary incontinence reduces quality of life. One survey found that women with urinary incontinence were nearly 3x more likely to suffer with depression: 2.2% in those without incontinence versus 6.1% in those with incontinence. Depression symptoms were worse for women with worse incontinence symptoms.
The risk of stress urinary incontinence is highest for all forms of vaginal delivery, with forceps posing the greatest risk. The chart below shows rates of urinary incontinence more than 1 year after birth.
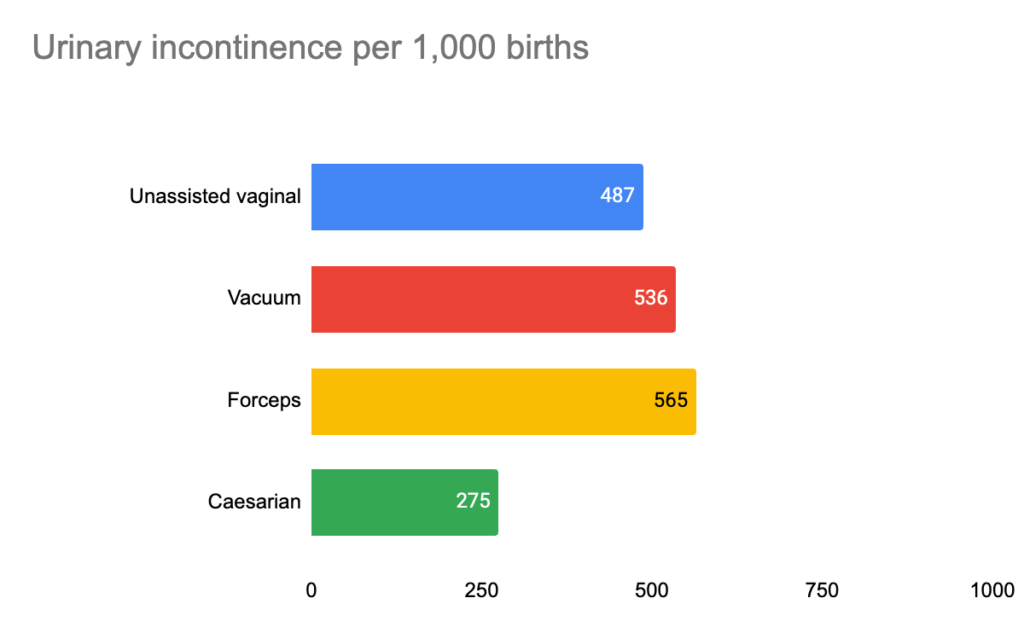
C-section poses the lowest risk of urinary incontinence. Out of 1,000 women choosing who give birth by forceps rather than c-section, an extra 290 will suffer urinary incontinence.
Pelvic organ prolapse
Pelvic organ prolapse occurs when some of the organs in the pelvis – the bladder, the uterus, or bowel – descends into the vagina. Many women who have pelvic organ prolapses are not symptomatic: they do not have the feeling of a bulge in their vagina.
Symptomatic pelvic organ prolapse has severe life-changing implications for women.
- Irreparable damage. The overarching feeling of women with pelvic organ prolapse is one of being irreparably damaged. Many women feel that their lives have been ruined by pelvic organ prolapse, and that there are no treatments available. Women with pelvic organ prolapse report lower quality of life.
- Constant discomfort. Many women with symptomatic pelvic organ prolapse describe feelings of constant discomfort, which severely disrupted daily life, such as pressure, heaviness, fullness, and the sensation that something was falling out of the vagina. Some women complained about vaginal flatus (‘queefing’), and an awful “open” feeling with a dragging sensation in the vagina. This constant discomfort was compounded by basic day to day activities such as cooking and walking, and even standing or sitting.
- Fear of physical activity. Many women with prolapse are afraid to do high-intensity sports, such as lifting weights or running, for fear that their symptoms might worsen. Women with prolapse are often afraid of lifting their children for the same reason.
- Sexual problems. Pelvic organ prolapse causes various various sexual problems, such as painful intercourse, lack of sexual pleasure and inability to achieve orgasm. For many, sexual intercourse no longer provided any pleasure and many complain of decreased vaginal sensation and vaginal looseness.
- Surgery. 10% to 20% of all women (not just those who give birth) will undergo surgery for pelvic organ prolapse. 30% of these women will require additional prolapse repair.
- Distorted body image. Many women with prolapse suffer from distorted body image and feel unable to see beauty in themselves. Women often feel disgust or embarrassment at their body.
- Psychological burden. Many women with prolapse find it difficult to think of anything else because they constantly feel prolapse symptoms, and are unable to return to forms of physical activity that they previously enjoyed. For many, the happiness of becoming a parent was overshadowed by prolapse.
For women giving birth vaginally, the risk of pelvic organ prolapse is large.
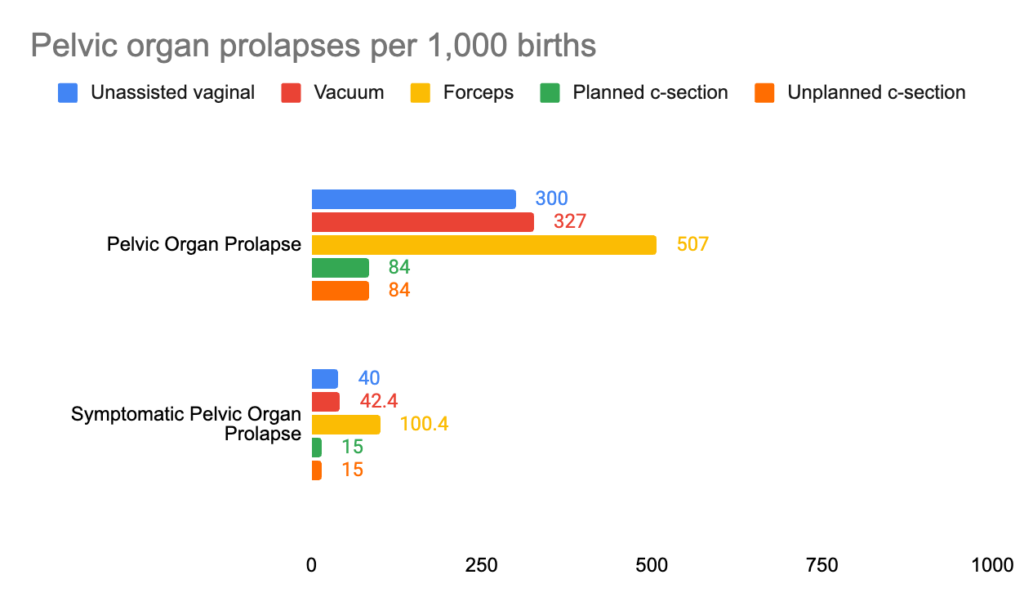
The risk of pelvic organ prolapse is greatest for forceps delivery: around 500 out of 1,000 women who deliver by forceps will eventually suffer a prolapse.
The risk is much lower for c-section: 84 out of 1,000 women giving birth by c-section will suffer prolapse.
Levator avulsion
A levator avulsion occurs when the pelvic floor muscle is pulled off the pubic bone. This is a long-term lifelong injury. Levator avulsion has important consequences for the wellbeing of women.
- Sexual dysfunction. The levator ani muscle is the main determinant of how ‘tight’ the vagina is, and so has been termed the ‘love muscle’ in the popular press. Levator avulsion causes reduced tone and loss of vaginal laxity. In surveys, more than half of women with avulsions say that they have to deal with long-term sexual dysfunction and relationship issues.
- Pelvic organ prolapse. Levator avulsion is an important risk factor for pelvic organ prolapse.
- Surgery success. The lifetime risk of surgery for pelvic organ prolapse is around 10-20%. Levator avulsion reduces the success rate of surgery by around a factor of 3.
The risk of avulsion for different delivery modes is shown below:
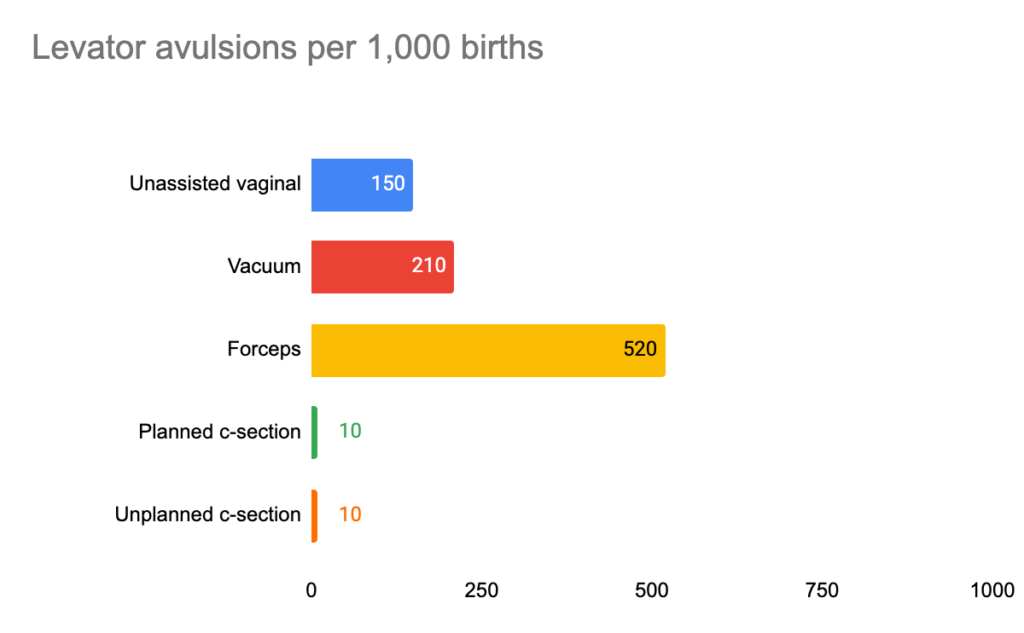
The absolute risk of levator avulsion for any form of vaginal delivery is very high. 150 of every 1,000 women having an unassisted vaginal birth will suffer a levator avulsion. Nearly half of women delivering by forceps will suffer an avulsion. C-section dramatically reduces the risk of levator avulsion.
Anal Sphincter Injury
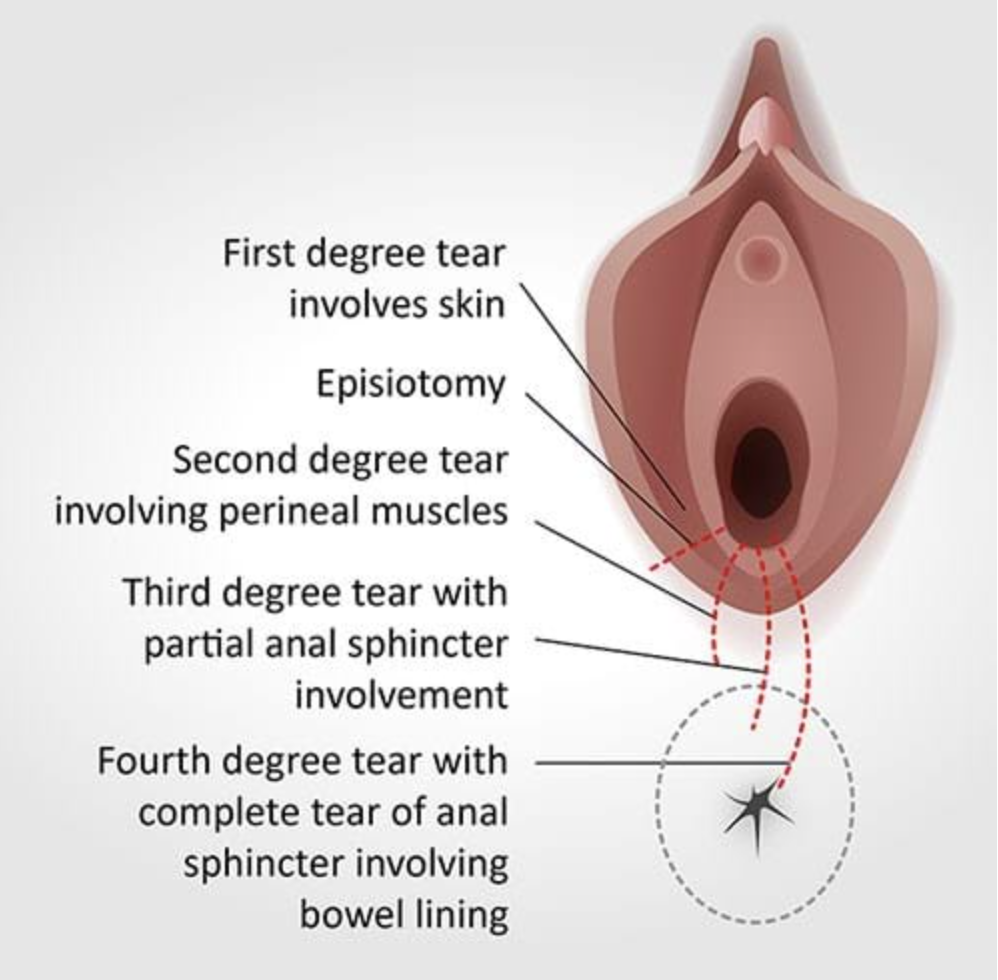
Tearing injuries are common in vaginal childbirth. What are known as ‘third and fourth degree tears’ involve injuries to the anal sphincter. The picture below shows the meaning of different types of tears:
Anal sphincter injuries impose a range of severe costs on women.
- Pain. Anal sphincter injuries are likely to cause pain when women go to the toilet.
- Fecal incontinence. Anal sphincter injuries are the most common cause of fecal incontinence, which is highly prevalent among women giving birth vaginally. 10-30% of women with anal sphincter injuries will develop fecal incontinence later in life. Fecal incontinence is discussed in more detail below.
- Sexual problems. Women with anal sphincter and perineal injuries may suffer pain during intercourse and sexual dysfunction.
- Other injuries. Severe anal sphincter injuries can lead to abscess formation, wound breakdown, and rectovaginal fistula – when there is an abnormal connection between the rectum and the vagina, which can allow gas or stool to pass through your vagina.
Surveys on the wellbeing effects of anal sphincter injuries identify the following themes.
“Extensive pain resulted in physical and psychological limitations and crushed expectations of family life.”
“Emotional impact… including grief, anxiety, shame, sadness and hopelessness”
“The psychosocial problems of negative self-esteem and personality changes associated with a change in body image for affected women are highlighted.”
“Isolation. Inability to function sexually. Anxiety about the future and future pregnancies. Seeing their body as injured.”
“Facing daily physical and psychological limitations. Living with crushed expectations. Difficulty navigating the healthcare system.”
“Women felt unclean which resulted in dignity loss, isolation, embarrassment, guilt, fear, grief, feeling low and loss of confidence”
“Social Impact: Delayed return to work, exercise restrictions, social limitations, relationship and family breakdown. Physical Impact: anal incontinence, faecal urgency, dyspareunia, prolonged postpartum recovery, pain and discomfort. Psychological Impact: distress of ongoing symptoms, effects on mental health, implications for intimacy and embarrassment. Healthcare Impact: Delay or avoidance of future births, surgical birth for future births, increased length of stay, risk of infections and complications, ongoing treatment and support and secondary repair”
The absolute risk of anal sphincter injuries are high for any kind of vaginal birth. The chart below shows the rate of anal sphincter injuries 15-24 years after birth.
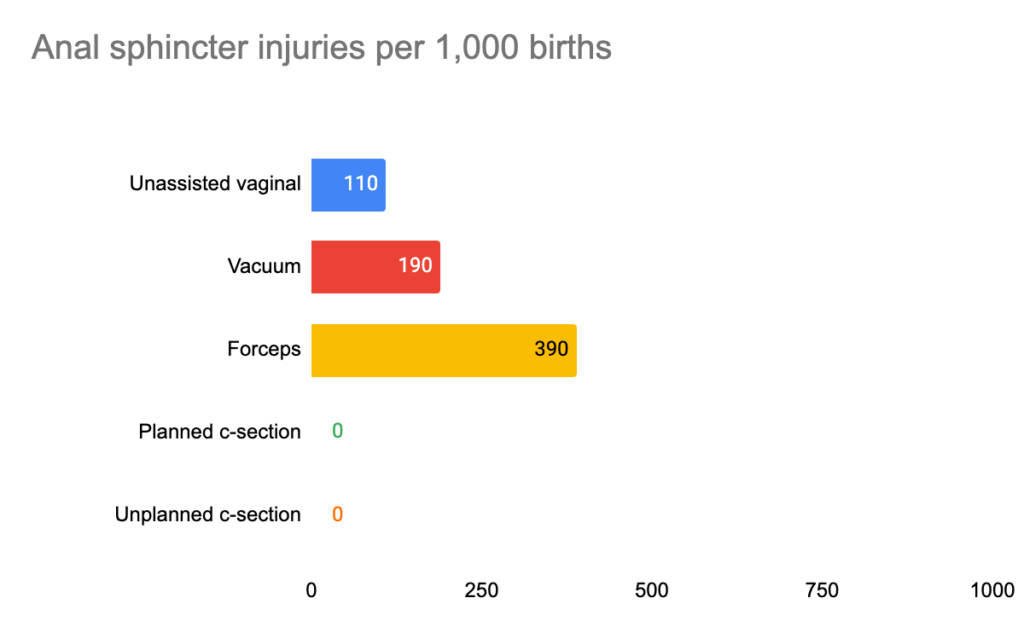
C-section eliminates the risk of anal sphincter injuries.
Fecal incontinence
Fecal incontinence includes a range of symptoms including passive soiling, or incontinence of liquid or solid stool (poo).
Fecal incontinence is a debilitating problem. People with fecal incontinence have lower quality of life, with negative impacts on lifestyle, coping depression and embarrassment. Around a fifth of women with fecal incontinence note a moderate to severe impact on quality of life.
The risk of fecal incontinence is high for all forms of delivery. The chart below shows the risk of fecal incontinence more than 5 years years after birth for different modes of delivery.
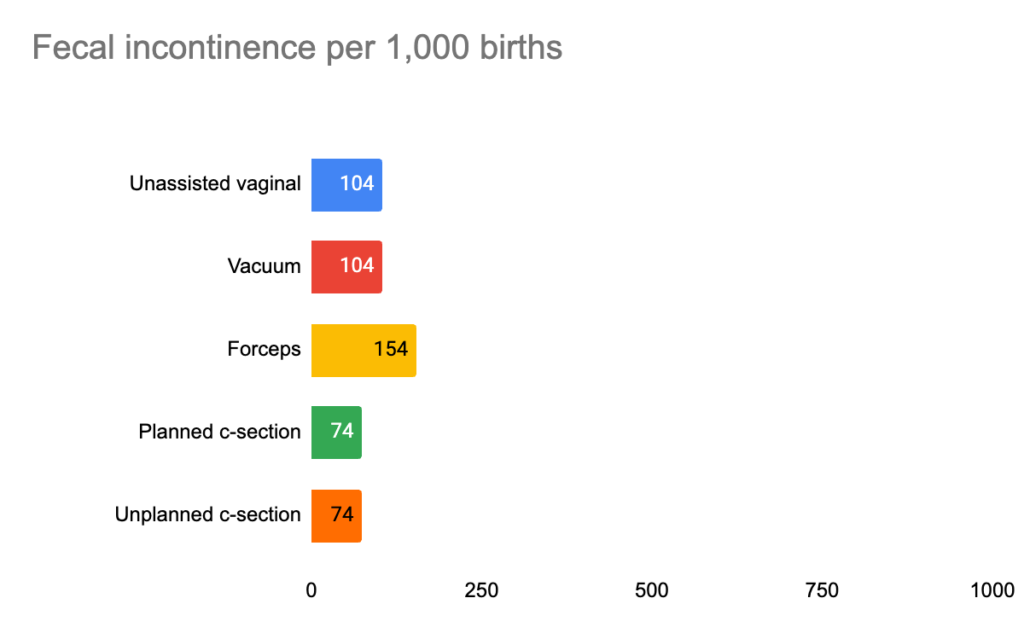
Forceps poses the greatest risk of fecal incontinence, and c-section the lowest. For 1,000 women giving birth by forceps rather than c-section, an extra 80 will have fecal incontinence.
Placenta praevia in future pregnancies
Placenta praevia is when the placenta completely covers the cervix during pregnancy. This means that the baby cannot be born vaginally and will have to be delivered by caesarian. Placenta praevia also poses serious risks to mothers and babies. If the placenta is still low in your womb towards the end of pregnancy, there’s a higher chance that you could bleed during your pregnancy or during your baby’s birth. This bleeding can be very heavy and put you and your baby at risk. Ananth et al (2003), a study of 22 million American births found that:
- The “Neonatal mortality rate was 10.7 with previa, compared with 2.5 per 1,000 among other pregnancies”.
- “At 28 to 36 weeks, babies born to women with placenta previa weighed, on average, 210 g lower than babies born to women without placenta previa.”
The risk of placenta praevia in subsequent births is low for all modes of delivery, but highest for c-section:
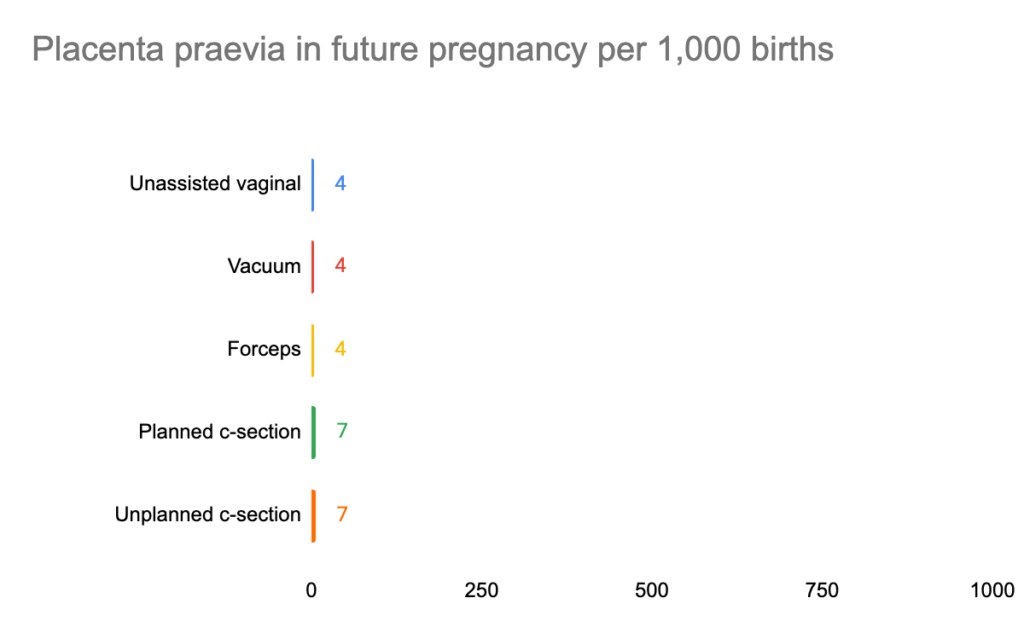
For every 1,000 women giving birth via c-section rather than vaginally, an extra 3 will suffer placenta praevia in future pregnancy.
Obstetric wound hematoma
Obstetric wound hematoma is a large bruise that can appear after birth. It is the most important risk factor for infection of wounds caused by birth, which we discuss below.
The risk of obstetric wound hematoma for all forms of delivery is low, but is highest for c-section.
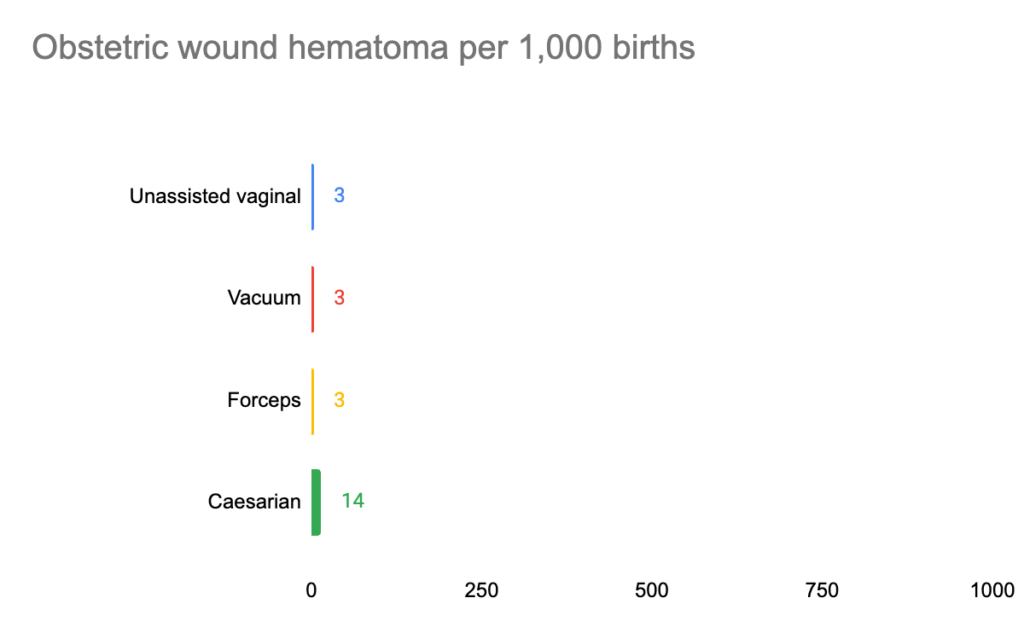
Out of 1,000 women choosing who give birth by c-section rather than vaginally, an extra 11 will suffer obstetric wound hematoma.
Rupture of womb in future pregnancy or birth
Rupture of the uterus or womb is a serious birth complication that occurs when your womb tears or breaks open. This can have life threatening implications for the health of both the mother and the baby. When your womb ruptures, the fetus is left without the protection of your womb. It can cause the fetus’s heart rate to slow down and leave it without oxygen. Without oxygen, the fetus is at risk for brain damage or suffocation.
The risk of rupture of the womb in future birth is mainly for women who had a c-section for their first birth but who decide not to have a planned c-section for their next birth (i.e. for their next birth, they have a vaginal birth or an unplanned c-section). The risk of womb rupture in future pregnancy is around 7 times higher for women who delivery vaginally for their subsequent birth than for women who have a planned c-section for their subsequent birth. Thus, the risk can be reduced dramatically by choosing to have an planned c-section for future births.
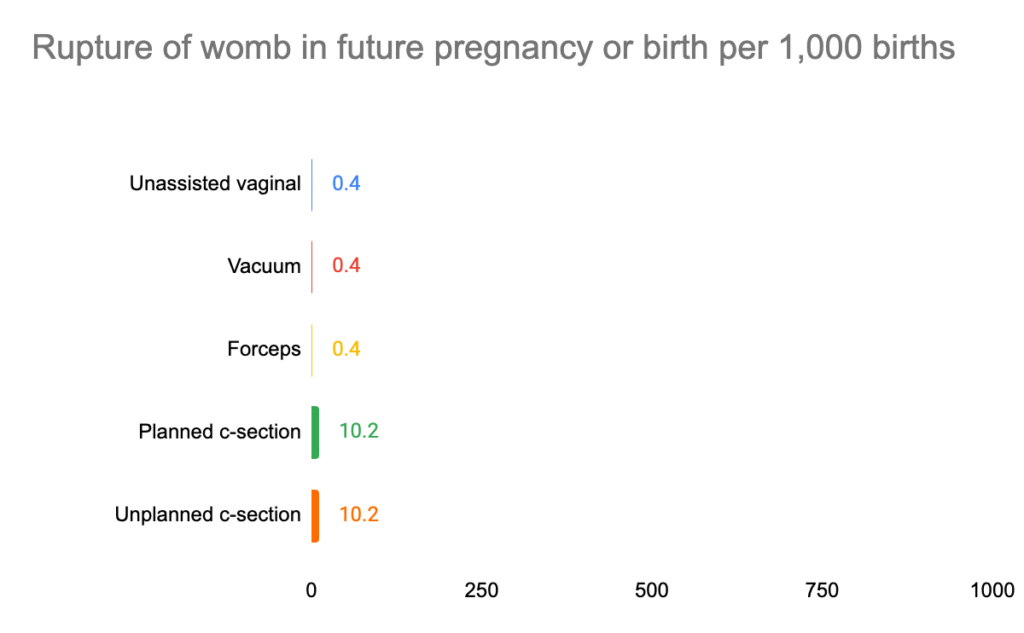
Out of 1,000 women who give birth by c-section, an extra 9 will have a womb rupture in subsequent pregnancies, though this risk can be reduced by having a planned c-section in future deliveries.
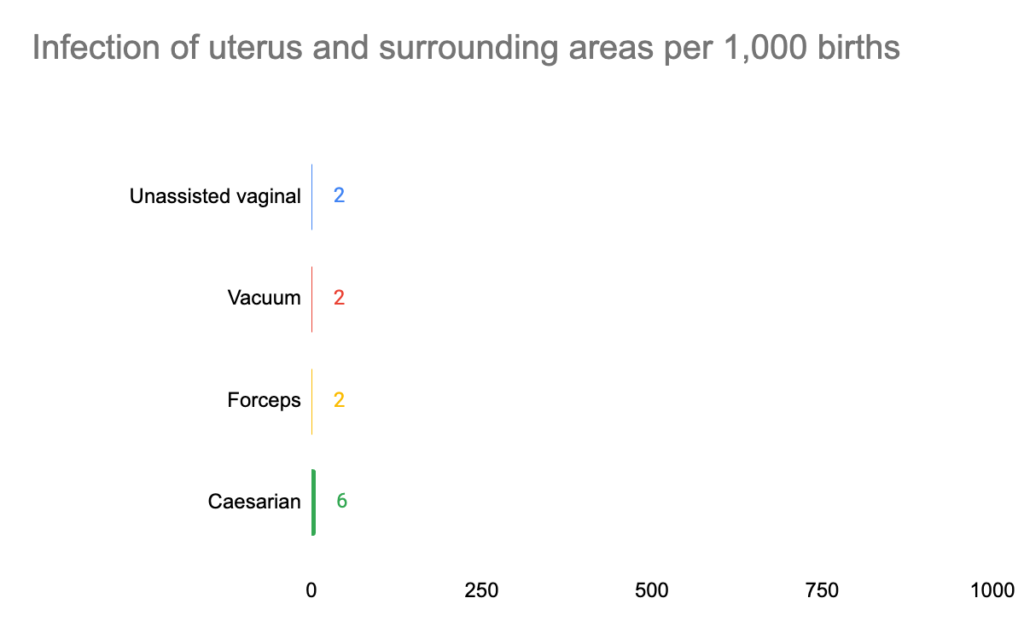
Infection of uterus and surrounding areas
Trauma sustained in vaginal or caesarian birth can become infected. Women experiencing infection may suffer from flu, chills and loss of appetite as well as suffering pain at the site of trauma. The risk of infection of the uterus and surrounding areas is small for all modes of delivery, but is highest for c-section:
Hysterectomy within 1 day of delivery
Peripartum hysterectomy is surgery to remove the womb within one day of delivery. This would prevent the possibility of having children in the future. The risk of hysterectomy within 1 day of delivery is very low for all modes of delivery, but the risk is highest for c-section:
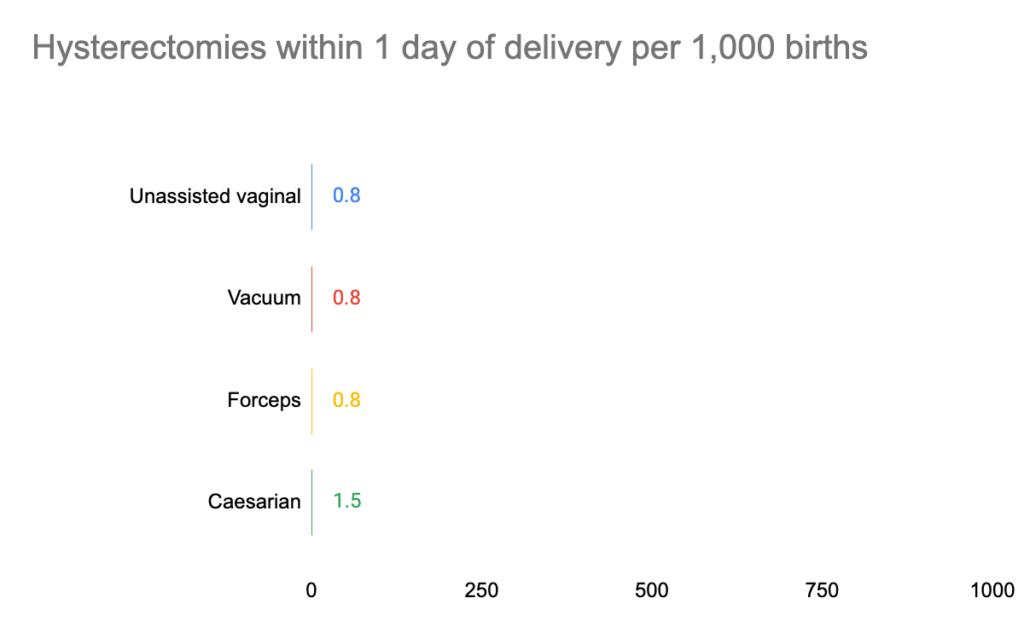
For every 10,000 women that give birth by c-section, around an extra 7 women will have a hysterectomy within 1 day of delivery compared to if they had given birth vaginally.
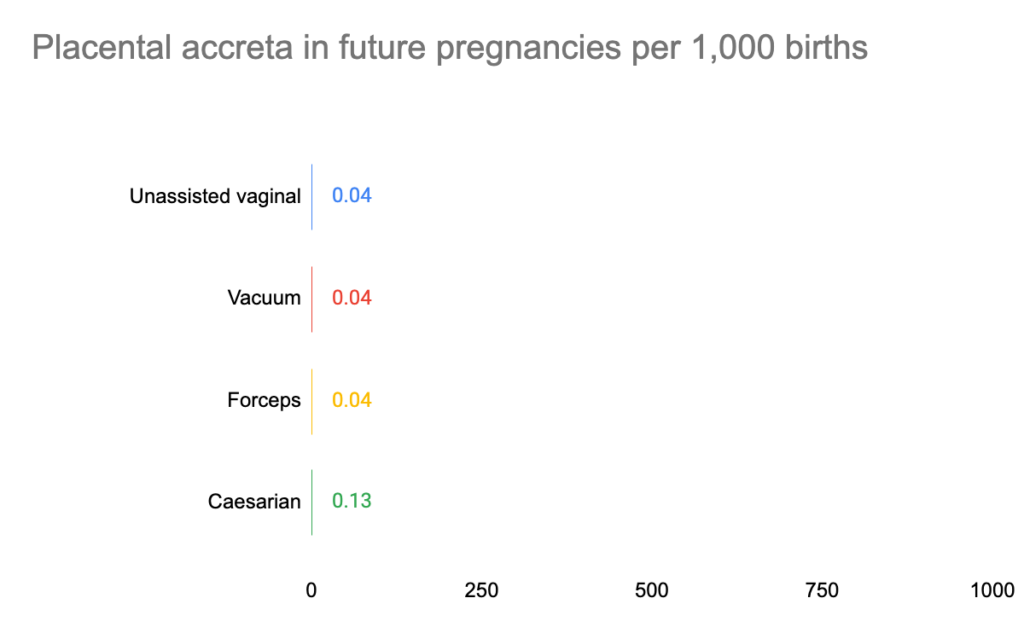
Placental attachment after childbirth
Placenta accreta is a serious pregnancy condition that occurs when the placenta grows too deeply into the wall of the uterus. Typically, the placenta detaches from the uterine wall after childbirth. With placenta attachment after childbirth, part or all of the placenta remains attached. This can cause severe blood loss after delivery.
Placental attachment after childbirth is considered a high-risk pregnancy complication. If the condition is diagnosed during pregnancy, you’ll likely need an early C-section delivery followed by the surgical removal of your uterus (hysterectomy).
The risk of placental attachment after childbirth is very low for all forms of delivery, but is highest for c-section.
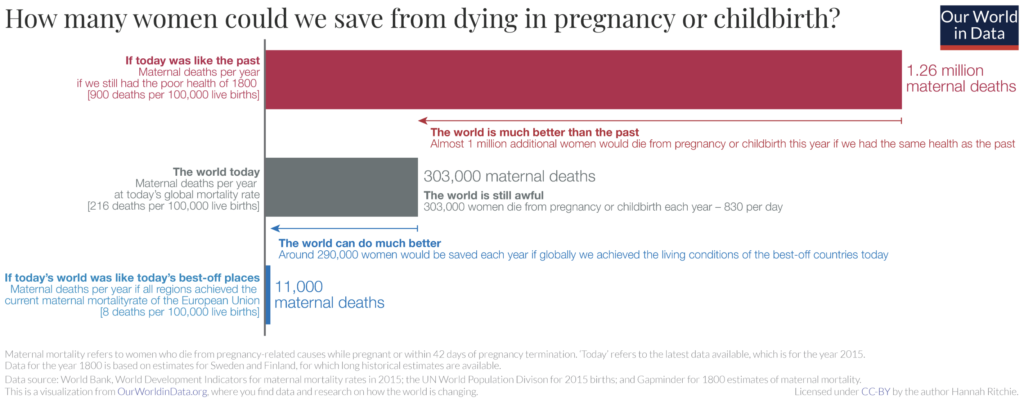
Maternal Death
Thankfully, in rich countries, maternal mortality is now extremely low and has declined enormously since the Industrial Revolution.
The chart below shows maternal mortality for planned vaginal birth and planned c-section. Note that planned vaginal birth includes all women who try to deliver vaginally. This could end in an unassisted vaginal delivery, but also in forceps, ventouse or unplanned c-section.
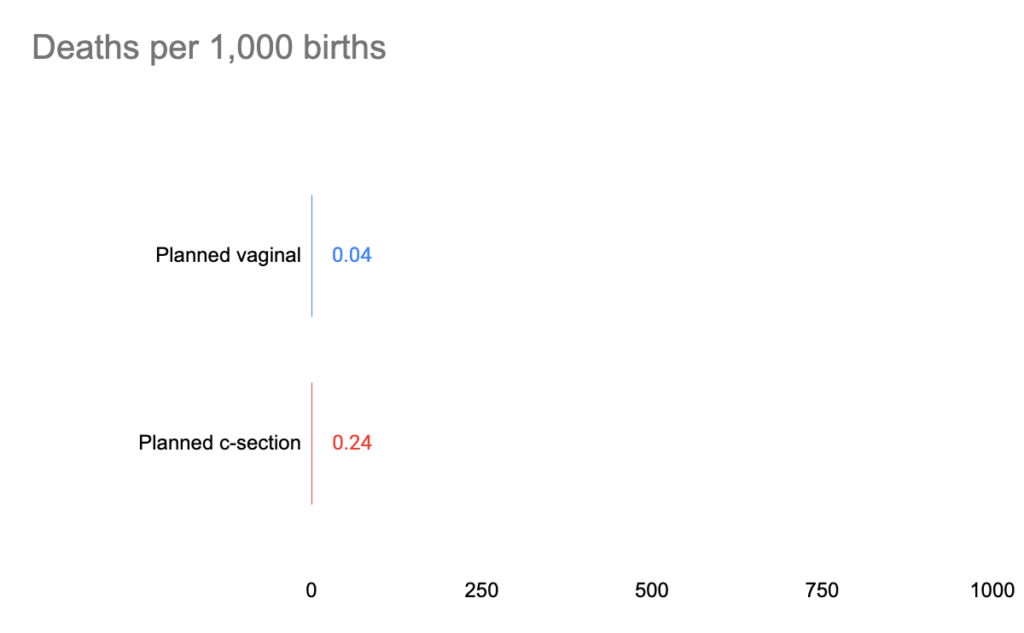
Women who deliver by forceps, ventouse or unplanned c-section are likely to face a higher risk of death than those delivered by unassisted vaginal, but that does not necessarily mean that those modes of delivery cause that increased risk. The reason for this is that forceps, ventouse and unplanned c-section are often done in order to prevent harm to the mother or baby, and so they might reduce the risk of death overall. (We discuss the issue of confounding in more detail on the supporting evidence page).
We think that due to confounding, it is not possible to provide reliable figures comparing the risks of forceps, ventouse and unplanned c-section to other modes of delivery in a way that doesn’t mislead. These procedures are often carried out because they are medically necessary.
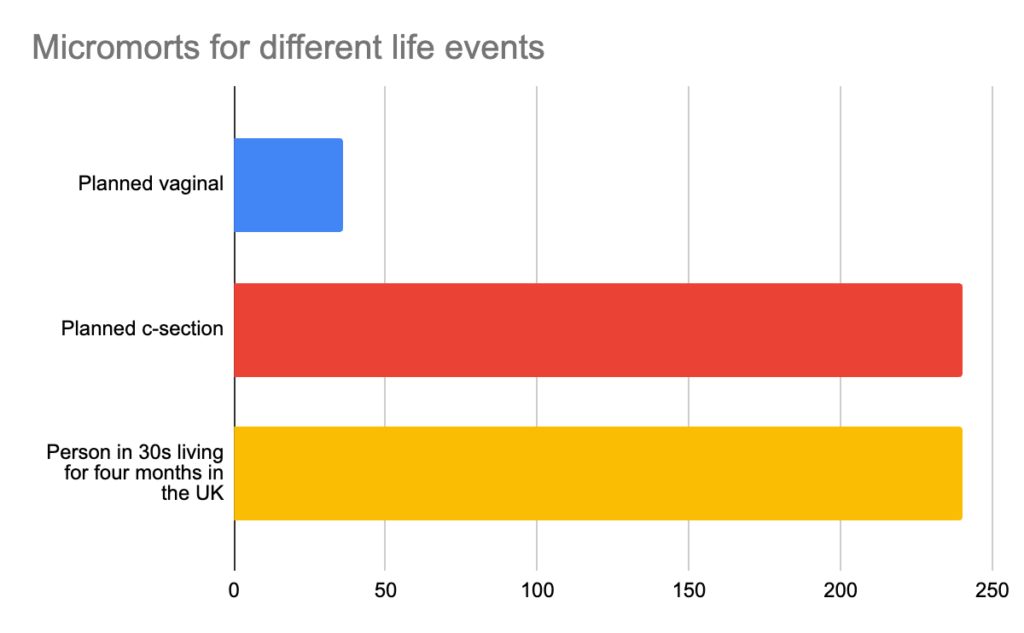
The small but important risks of death can be hard to wrap your head around. One way to get some perspective is to compare this risk to levels of risk that people face in their ordinary lives. ‘Micromorts’ are a useful way to get a sense of risks of death. A micromort is a one in a million chance of death. A typical person in their 30s in the UK experiences around 2 micromorts per day. This is 730 per year.
Having a planned vaginal delivery exposes you to 36 micromorts, or around the risk of death a thirtysomething in the UK would face living for 18 days. Having a planned c-section exposes you to 240 micromorts, or around the risk of a thirtysomething in the UK would face living for four months.
Giving birth increases your risk of death significantly, but these risks are not very large in absolute terms, and are comparable to ordinary risks we routinely face.